|
Why Did The FDA Greenlight
The COVID Vaccines?
Recent
whistleblower testimonies have revealed the anatomy
of corruption within the FDA
The
medical field has always had a problem holding onto dogmatic traditions
and attacking physician dissidents who risk their careers to point out
why those practices are unsafe and ineffective. To address this, in the 1960s,
physicians began pushing for medical practice to be dictated by
scientific evidence rather than entrenched interests, and in 1991, “evidence-based medicine”
was born.
This
mindset quickly caught on and overturned many disastrous medical dogmas,
but unfortunately, gradually succumbed to the same issues that had
created it in the first place, with “evidence-based medicine” becoming
its own dogma and the rest of the medical system (e.g., pharmaceutical
dollars) restructuring itself to provide more and more fraudulent
evidence to sustain the current dysfunctional medical dogma while
simultaneously attacking any contrary views as “pseudoscience” “lacking
evidence.”
Note: much of this is a result of RCT fundamentalism (a belief that
only prohibitively expensive large RCT’s can constitute “evidence”)
despite the fact those expensive trials are notoriously for consistently
finding results that favor their sponsors and a 2014 Cochrane review proving
that smaller (affordable) observational trials will get the same results
as larger RCTs. Likewise, there’s a widely held belief that data is only
valid if published in a major journal despite those journals having
massive financial conflicts of interest, which cause them only to publish
things that reinforce their existing narratives.
In
turn, one of the main reasons this publication exists is that the harms
of many routine medical practices significantly outweigh any benefits
they provide. However, despite decades of evidence showing this, the
medical system has continued to hold onto them. For example, in this
publication, I have covered massive issues with:
•NSAIDS, Opioids,
and Gabapentin for
pain relief.
•Spinal surgeries for
neck and back pain.
•Benzodiazepines for
anxiety
•SSRI Antidepressants for
depression
•Sleeping pills for
insomnia
•Stomach acid blockers for
acid reflux
•Statins to
prevent heart disease
•All of the blood
pressure medications
• Osteoporosis medications (e.g.,
Fosamax)
•Ozempic for
weight loss
•The HPV vaccine for
cervical cancer
•Hormone blockers for
blocking puberty of gynecologic issues
•Tamiflu and flu shots to
treat the flu.
Sadly,
while each of those stories is outrageous (particularly since safe and
effective treatments already exist for those conditions), they barely
scratch the surface, as there are so many established medical practices
the existing evidence strongly argues against to the routine use of. Even
more troubling, these issues escalated dramatically during COVID-19, as
any semblance of evidence-based decision-making was swiftly abandoned in
a frantic rush to implement one profitable yet detrimental intervention
after another while countless therapies that could have treated COVID
were rapidly abandoned.
Because
of that rapid escalation, many everyday physicians were put into a
position where they could either go along with much of what they’d been
trained to do being thrown out the window or speak out and be branded as
a radical far-right extremist (despite holding views that had been
mainstream beliefs in medicine until just a few years ago).
Note: beyond the well recognized physicians who spoke out against the
COVID-19 policies and were targeted for doing so,
many more doctors (e.g., including some I knew personally) did as well,
but did not attract national attention since they had smaller platforms.
The Forgotten Side of Medicine is a
reader-supported publication. To receive new posts and support my work,
consider becoming a free or paid subscriber. To see how others have
benefitted from this newsletter, click here!
Subscribed
Philip Krause
One
of the most important whistleblowers to come forward was Philip Krause,
who had worked in the FDA for 30 years. This was because Krause along
with his direct superior Marian Gruber, had been the most senior FDA
officials in charge of America’s vaccines, and at the end of August 2021,
in the middle of arguably the FDA’s most critical vaccine assessment in history, they abruptly resigned (which
was a seismic enough event the mainstream media covered it and even
mentioned it being due to political pressure from White House for the
COVID boosters). Following this, Krause and Gruber published an article in the Lancet.
Krause also published a series of editorials (e.g., this one, this one, this one in
the Washington Post) arguing against the current booster program.
Following
this, he testified in front of Congress about how the COVID vaccines were
handled.
Note:
Dr. Gruber also provided information to the Congressional Committee.
Most
recently, he was interviewed by Rav Arora (who authors The Illusion of Consensus on
Substack) and provided an even more in-depth summary of what happened.
Collectively, Krause’s testimony highlighted a few
critical points.
First,
as I discussed in a previous article,
in 2022, Congress’s watchdog, the Government Accountability Organization
(GAO), investigated aspects of the COVID-19 response. This included
scientific integrity within the four major branches responsible for the
response (CDC, NIH, FDA, and ASPR). From interviewing employees in each
agency, the GAO found that
political interference repeatedly overrode government scientists
following the available science and that employees in each agency rarely
reported it as they felt their supervisors were already aware of it and
that no whistleblower pathways existed in any of the agencies (which is a
huge problem). In contrast, their superiors denied all of this and disingenuously
argued that the lack of reports of violations of scientific integrity
meant no violations were occurring.
While
these are quite heavy allegations to direct against the government, in my
eyes, Krause’s testimony provides the most substantial proof we have that
this scientific interference was happening, and if anything was
systemic.
Second,
Krause is very pro-vaccine (e.g., he presided over other vaccine debacles
at the FDA, and after leaving the FDA he’s continued to work for the
vaccine industry). As such, his resignation and him publicly speaking out
about the FDA’s actions (which almost never happens) demonstrate
just how bad the FDA’s conduct was.
Third,
throughout COVID-19, many felt our healthcare authorities lied to us
(even as the media claimed otherwise). Krause’s testimonies not only show
that this was the case, but also that America’s political leadership had
an incredibly poor understanding of the vaccines they were promoting and
nonetheless chose to keep on doubling down on them regardless of what
evidence was brought forward (e.g., that the vaccines did not prevent
transmission).
Finally,
the GAO report was not the only indication that something
was seriously amiss at the FDA.
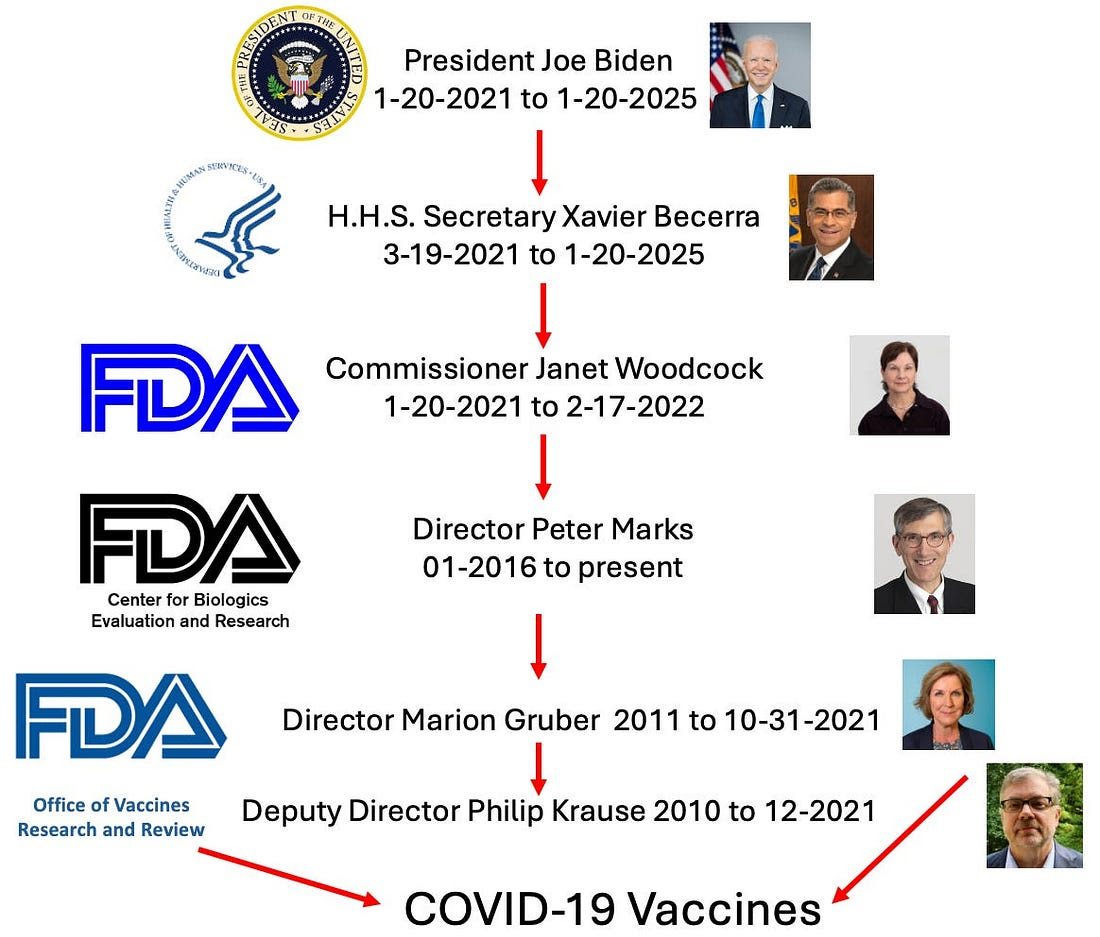
The FDA’s Leadership
If you
know the key individuals involved, much of what follows will be much
easier to understand.
|
|
Duplicated
|
Note:
this is a small snapshot of the Federal Government (e.g., H.H.S. oversees 13 agencies including
the CDC, the FDA has six Centers and several offices, the FDA’s Center
for Biologics has six offices including one for vaccines, which has a
couple hundred employees).
Concerning
these individuals, it’s worth mentioning that:
•Biden
and many of his staffers were directly responsible for the unconscionable
vaccine mandates pushed on America and the demonization of the
unvaccinated—much of which were based on things that were known to be lies at
the time Biden announced his mandates.
•To
my knowledge, none of us were ever able to reach Xavier Becerra.
•Janet
Woodcock (to her credit) engaged limited communications with the vaccine injured (where she was
repeatedly informed about the severe injuries many had experienced) and
did a bit to have their injuries be evaluated (e.g., see this Congressional testimony and NYT article) but
admitted she did much less than she felt she should have for them
(possibly due to political pressure from above). Additionally, Steve
Kirsch reached her, but she dismissed his concerns about COVID vaccine
data as misinterpretation without ever explaining how.
•Peter
Marks repeatedly communicated with those injured by the COVID-19
vaccines. He expressed empathy with what they were going through, but
consistently set impossible benchmarks for any of their injuries to be
linkable to the vaccines regardless of the evidence presented to him
(e.g., see this leaked recording).
•No
one in my network was able to reach Marion Gruber (despite directly
contacting her), but Gruber did testify to Congress about the issues she
observed throughout the approval process.
The COVID-19 Vaccine Approval Timeline
Since
pharmaceuticals typically take 10-15
years to bring to market, it was unlikely one could be
appropriately brought to market before a natural herd immunity to
COVID-19 set in. To bypass this, three steps were taken:
•Vaccine companies were paid to
make their vaccines before it was proven effective and safe, so that when one of them was approved, a supply
would already exist that could be distributed (rather than waiting for it
to be produced). Likewise, a system was implemented so they could
be rapidly distributed the moment they were approved.
•An
alternative approval process (an Emergency Use Authorization or EUA) was
put into place that allowed the vaccine to be “approved” if preliminary
evidence showed it might help under the condition that it would then be
extensively tested for safety later on (which, as you might guess, never
happened).
•
Many corners were cut to expedite the approval process, which proved
problematic (e.g., poor production resulted in highly variable vaccine
lots, which were often more dangerous or contaminated with
synthetic bacterial DNA).
Because
of these issues, many were concerned about the vaccines (e.g., the editor
of a leading medical journal published a series of ignored
editorials in 2020 that accurately identified many of
the significant issues with the COVID-19 vaccines). More remarkably, due
to the political polarization of the time, many prominent Democrats
(e.g., Kamala Harris and Joe Biden)
stated they had immense distrust of “Trump’s Vaccine” but once the first EUA came out, they flipped and
instead became its most ardent proponents.
Note:
during COVID-19, while the Trump administration initially tried to
explore alternative therapies for COVID-19 (which would have ended the
pandemic), due to the pushback they received from the media (e.g., with
hydroxychloroquine), they eventually settled on doing everything they
could to get a vaccine to market before the election. One of the most
remarkable things about this was that at the last moment, Pfizer bumped its approval back,
to right after the election, which arguably cost Trump the
election. Fortunately, it also greatly damaged Pfizer’s standing
with the Trump administration (which I suspect is one of the reasons why
RFK Jr. has been able to overtly challenge the pharmaceutical industry).
At
the time the Pfizer and Moderna’s vaccines received their initial EUA,
they were claimed to be 95% effective, and an almost religious jubilation
passed through the medical field (e.g., I heard many people say “we’d
hoped they’d be effective, but we never imagined they would be that effective”).
Despite many serious issues with the vaccines, the belief that vaccines
were our salvation was so powerful that I quickly realized it was a lost
cause to warn my colleagues about it (even some who’d previously had
concerns about other vaccines).
Note:
this was primarily due to the vaccines being marketed based on, nothing
else working for COVID and us hence needing to lockdown until the
vaccines came out, which made individuals very receptive to vaccinating
so “things could return to normal.”
These
claims however, were lies. This was partly due to statistical
manipulation (e.g., on 1/4/21, immediately after the Pfizer’s trial was
published, the BMJ pointed out the
vaccine’s actual efficacy was 19%—thereby making it ineligible for an
approval) and partly due to outright fraud as whistleblowers showed all
the major vaccine manufactures concealed a myriad of severe reactions to
their COVID vaccines and a trial supervisor for Pfizer
pointed out their trial was not blinded and was
deliberately inflating the efficacy of Pfizer’s vaccine. Furthermore, it
was well known that the SARS-CoV-2 virus was rapidly mutating, so any
benefits created by the vaccine were likely to be short lived.
Note:
one of the biggest lies that emerged at this time was that the COVID
vaccines stopped viral transmission (which in reality they had never been
tested for, and based on the vaccine’s design was unlikely to happen).
As
such, once the “safe and effective”
vaccines came to market, the vaccines (like many before them)
quickly failed to perform as promised, so the goal posts were rapidly
shifted and before long the vaccines only “prevented severe illness and
death” (much of which I believe was due to inaccurate hospital
data erroneously stating hospitalized COVID patients
were unvaccinated).
Because
of the mounting injuries and repeated vaccine failures, the public became
more reluctant to vaccinate. To combat this, a series of increasingly
aggressive measures (e.g., bribes and then exclusion from social events)
were implemented to sustain vaccine sales. However, by summer 2021, it
became clear this would not work, so the next phase (mandates and
boosters) was pivoted too. This in turn, required a formal FDA approval
for at least one vaccine and an approval or EUA for at least one booster.
Unfortunately,
the existing evidence did not support this, to the point that the staunch
supporters of vaccination, Dr. Krause
and Dr. Gruber (our two top
vaccine experts) felt they could not go along
with it as:
•The
existing data showed that while general immunity from the COVID vaccines
was disappearing (as the virus had mutated), it was still protecting
against death. As such, since the only thing the boosters (which were
identical to the original vaccines) could do was protect against death,
there was no point in giving boosters to individuals who had already been
vaccinated or had already had COVID-19 (and who were not at high risk of
a severe COVID-19 infection).
Note: they also highlighted that the lack of booster efficacy at
preventing infections from the current strains (seen throughout the
existing literature) was likely due to the booster not matching the
current strain.
•Since
vaccine supplies were still limited, it made much more sense to give them
to those who were unvaccinated and could benefit from them rather than to
boost those already vaccinated.
•Giving
boosters such a short time after the initial vaccines would shake public
trust in the original vaccines and undermine vaccination efforts (as
pivoting from “95% effective” for life to “stops working after 8 months”
does not inspire confidence). Additionally, it could
create distrust with the rest of the vaccine program if injuries
followed.
•Some
“rare” side effects (e.g., myocarditis or Guillain-Barre syndrome) had
been detected from the vaccine, which became more frequent with
successive doses.
Let’s
now look at what transpired.
Note:
much of what follows is further detailed within this Congressional report.
Pfizer’s Vaccine Approval
On
May 18, 2021, Pfizer submitted an application for licensing of its
vaccine. Under normal circumstances, this review would take around 12
months to complete, but due to it having a priority review status, that
was shortened to 8 months (resulting in an expected approval around
January, 18, 2022). This was a considerable problem for the FDA
leadership (and the Biden administration) as they needed the approval
much earlier.
Because
of this, Gruber and Krause began being subjected to continual pressure to
find a way to accelerate the approval of Pfizer’s vaccine, while their
repeated pleas to their superiors (e.g., Woodcock and Marks) not to do
this were ignored. Initially, they set the approval for mid-October 2021,
but after significant pressure from Marks, they agreed to shorten it to
September 15.
Following
this, Marks said that was still too long (which Krause felt suggested
pressure from outside the FDA caused Marks to change his timeline), and
demanded it be shortened further. Immediately afterwards, on July 15
2021, Gruber emailed Marks to (accurately) explain why that would not be
possible without “cutting corners” and why doing so was likely to
create a significant number of issues such as:
•Destroying public trust in all vaccines.
•Diverting FDA staff from other critical projects.
•Interfering with the necessary review for concerning symptoms that were
emerging or determining how different groups (e.g., the children and the
immunosuppressed) responded to the vaccine.
•Prevent the FDA from doing in house testing of the vaccines (which was
standard procedure for novel vaccines and likely would have caught many of the poorly produced
hot lots we saw after their rushed mass production).
Marks
then forwarded the email to Dr. Woodcock to ask for a phone call to
discuss the situation, to which she instead stated she wanted Marks to
take over the vaccine approval, and on the 19th she
convened a meeting with the four of them at which point Gruber and Krause
were taken out of their leadership role on the vaccine approval.
Note:
Krause stated that their removal from the approval was highly unusual
(e.g., in the entire time he’d been at FDA, he’d never seen anything
similar.
Marks
did as asked, and Pfizer’s vaccine was ultimately approved on August 23,
2021, for everyone 16 and above. Vaccine mandates then began being
enacted (starting with the military on
August 24, 2021, along with New York City around that same time period).
Given
that the FDA’s two most experienced vaccine reviewers felt that fast of
an approval was impossible (and furthermore they were excluded from
participating in or managing the review process) I believe it is fair to
assume many critical steps were skipped in a review process which
ultimately took a third to a half as much time as it should have. In
turn, after extensively investigating the events that transpired, the Congressional Oversight
Committee concluded that this accelerated timeline
was done to enact those Federal, state, and workplace mandates and was a
result of significant pressure from the Biden administration to ensure
their target mandate date could be met.
Note:
on July 8, 2022 the
FDA fully approved Pfizer’s vaccine for children ages 12-15, while on
October 29, 2021, it gave an EUA for children 5-11, and on June 17, an
EUA for children 6 months to 4 years of age. These approvals are
noteworthy, as young children have close to a 0% risk of dying from COVID
(making it difficult to categorize it as an “emergency” requiring an EUA).
At the same time, the existing vaccine schedule gives infants multiple
COVID vaccines in the first few weeks of life (despite vaccines not being
FDA-approved). Likewise, college students were required to get boosters
despite having no FDA approval.
Booster Approval
On August 18, 2021,
the Biden and the H.H.S. leadership (including Dr. Woodcock) announced a
plan to offer all Americas booster shots on September 20, despite neither
the FDA or CDC review times (or their advisory panels) having yet come to
a conclusion on if the boosters should be recommended, nor Pfizer or
Moderna having applied for the boosters (after which several months would
normally be needed to review the applications). Shortly after Dr. Gruber
(on 8/27) and Dr. Krause (on 8/30) submitted their resignations (but
continued to work at the FDA.
Note:
Krause stated he resigned because he could see outside interference
short-circuiting the approval process, resulting in him being constantly
overruled whenever he tried to do his job.
On August 31, 2021,
The New York Times reported that Dr. Gruber and Dr. Krause would leave
the FDA by the end of September. Both were reportedly unhappy with the
Biden administration's recent recommendation that adults receive a
COVID-19 booster eight months after their second shot, believing there
wasn't enough data to support the decision. They also saw the
announcement, which President Biden strongly promoted, as pressure on the
FDA to approve booster shots quickly.
On September 13, Dr.
Gruber and Dr. Krause (and 16 other scientists) wrote an article in the
Lancet that used the existing data to strongly criticize the COVID-19
boosting program and said boosters were only appropriate for specific
high-risk groups.
Note:
on May 13, 2024,
Dr. Janet Woodcock stated that she never read that article as she “was
very well aware of all the data.” “I know these folks, and I did not feel
the need to read their argument.”
On September 17,
the FDA’s advisory panel voted against authorizing a booster for the
general population, and then in a subsequent vote, authorized it only for
high-risk groups, including those in “high-risk” occupations (which the
FDA enacted on September 22).
Note: after publication of the September 13 article, Dr. Marks removed
Dr. Gruber from managing the advisory panel and thus directed the
September 17 meeting where he invited Israeli researchers to present
booster data to the committee they had not been provided with beforehand
(which was highly unusual) and had significant issues that overestimated
their benefits.
On September 23,
the CDC’s ACIP voted to recommend the booster for high-risk groups, but
unlike the FDA, felt “high-risk” occupations (e.g., being a teacher or
healthcare worker) did not need the vaccine. However, the next day, in a
“highly unusual” decision (which came as a surprise to her
staff), the CDC’s director overruled its panel and
recommended the boosters to “high risk” workers as well.
During
ACIP’s meeting, experts who voted against the measure argued that there
was insufficient data to support the recommendation, that it was too
narrow and premature, and that there was little marginal benefit in
acting then rather than waiting for better data. They also said that they
felt they were being pulled into an “emotional decision” and that this
decision could undermine confidence in the primary vaccine series.
Restoring Transparency
In
speaking out, Dr. Krause has repeatedly emphasized the importance of
restoring trust in the Federal Health Agencies and highlighted how the
conduct we saw throughout the COVID-19 vaccine campaign was incredibly
detrimental to that trust.
In
turn, he argues that:
•The
decisions made at the FDA must be transparent, particularly those
relating to EUAs (e.g., breaking down exactly how a novel therapy
qualified for that designation).
•If
independent advisory committees are not allowed to make decisions on
approvals or vaccine requirements, it dramatically undermines the
public’s trust in them.
•Individuals
who have a vested interest in determining a regulatory outcome must not
be put into positions of power at the agency (which amongst other things,
is why the system was structured so that the FDA approves vaccines but
the CDC recommends them).
•There
needs to be a robust appeals process that allows scientists who were
politically overruled by their supervisors to challenge that decision, as
the immense power senior FDA leaders wield to overrule review teams has a
corrosive effect on the agencies credibility.
Note: Krause also cited Peter Marks overriding a FDA review team in
2024 to approve a multi-million dollar gene therapy that failed its clinical
trials, and a similar event happening in
2016 where Janet Woodcock (not yet the FDA director)
overruled another FDA team. Likewise, in 2021, after the FDA’s panel
voted against approving a controversial Alzheimer’s drug (as it didn’t
work but caused brain bleeds), FDA leadership (including
Peter Marks) overrode the panel and approved the drug, which led to
members of the panel resigning, others labeling it the worst drug
approval in history, congressional investigations, and the costly drug
ultimately being taken off the market because no one wanted to use it.
Conclusion
While I agree with many of Dr. Krause’s points
(excluding that the vaccines were fairly safe and effective), I also
believe he ignored a more significant issue.
Ethically,
it is tough to justify a vaccine mandate, and as such, if it is done,
great care must be taken to ensure it has a very strong justification. In
contrast, it would be terrible to mandate a vaccine that:
•Provides no benefit to either the vaccinated individual or those around
them.
•Has a high enough injury rate that over half of the country
believes they are dangerous.
• Used for an easily treatable illness that does not pose a significant
risk to most of the population.
•The population did not feel their leaders were truthful or transparent
about.
As
each of those applied to the COVID-19 vaccines, it was a foregone
conclusion that there would be a massive loss of trust in our medical
authorities, and to some extent the political class and mass media as
well. At this point, while efforts are starting to be made to restore
that trust, I still do not believe most of our political leadership or
the medical profession grasps just how much trust has been lost or that
the old playbook (berating people with and endless stream of “experts”)
will no longer shift things.
Note: this is best demonstrated by a recent large JAMA study which
found in April 2020 that 71.5% of American adults trusted doctors and
hospitals, but in January 2024, only 40.1% did—which is a genuinely
profound loss of trust.
In
turn, I hope that this profound loss of trust (and the alternative
medical sales it creates) will begin forcing the medical system to start
providing actual transparency (e.g., currently we are not allowed to see
most of the data that determines if a drug will be approved) and switch
to promoting medical products that help people rather than profitable
ones that harm them. For example, as I show here, much in
the same way the FDA has forced through through unsafe and ineffective
treatments, over the decades, it has also gone to extraordinary lengths
to suppress many different remarkable therapies which would have
completely transformed the practice of medicine and greatly helped a lot
of people (but could not be allowed to enter the market as they would
have outcompeted the unsafe and ineffective therapies the FDA approved).
Fortunately,
the immense greed of the pharmaceutical
industry was enough to wake the world up (e.g., here I showed that
the nation’s two top vaccine scientists accurately predicted many of the
issues that would arise from rushing the vaccines through but nonetheless
were sidelined because they were getting in the way of vaccine sales) As
such, we now live in an unprecedented time where previously impossible
things that can actually shift things (e.g., the MAHA movement and RFK
Jr.) are beginning to appear. In order to make something of this moment,
permanent shifts will need to be made within our institutions. Because of
this, it is my hope that this dissection of some of the corruption we
witnessed throughout COVID-19 has provided some helpful insights into
what needs to be addressed (e.g., Peter Marks is still CBER’s director)
while we have the window to change it.
I
cannot describe how disheartening it has been to work with the FDA over
the years (e.g., quite a few of us were repeatedly stonewalled when we
tried to get the FDA to look at already available treatments for
COVID-19). For that reason, I am incredibly grateful a once-in-a-lifetime
opportunity has been created that can shift much of this and for all of
your support, which has made it possible for me to be a part of making
this change happen.
The Forgotten Side of Medicine is a
reader-supported publication. To receive new posts and support my work,
please consider becoming a free or paid subscriber.
Subscribed
Click below to share this post!
Share
To learn how other
readers have benefitted from this publication and the community it has
created, their feedback can be viewed here.
Additionally, an index of all the articles published in the Forgotten
Side of Medicine can be viewed here.
Invite your friends and earn rewards
If you enjoy The Forgotten Side of
Medicine, share it with your friends and earn rewards when they
subscribe.
Invite Friends
© 2025 A
Midwestern Doctor
Substack Inc., 111 Sutter St 7th Floor, San Francisco, United States
94104
Unsubscribe
|
